Enquiry Sent to the Office for National Statistics (ONS) Regarding ‘Missing’ Deaths in the United Kingdom
 Filed under:
Filed under:  he December undercount was last mentioned here 7 days ago. It still has not been corrected, so I’ve E-mailed the relevant department of ONS:
he December undercount was last mentioned here 7 days ago. It still has not been corrected, so I’ve E-mailed the relevant department of ONS:
Dear Sarah Caul,
I have been tracking ONS data very closely for about a year and I wrote over 100 blog posts about it. Thanks for the relatively (compared to other countries) rapid data disclosure on deaths per week. Corporate media does not need to lie about the data if it can relay false narratives and spin. That’s why people should not rely on the media; check the data. I go by the data. My Ph.D. was in Medical Biophysics, focusing on statistics.
Political intervention is always a threat. You proudly disclose you’re not subjected to political influence. This is great news.
I rely a lot on (and appreciate) the data you release every Tuesday morning at around 10AM. Hence, the integrity of the data is important to me. Editorialising it and repeating government communication strategies (debunked online) distracts from the core data. So I try to stay away from the textual stuff.
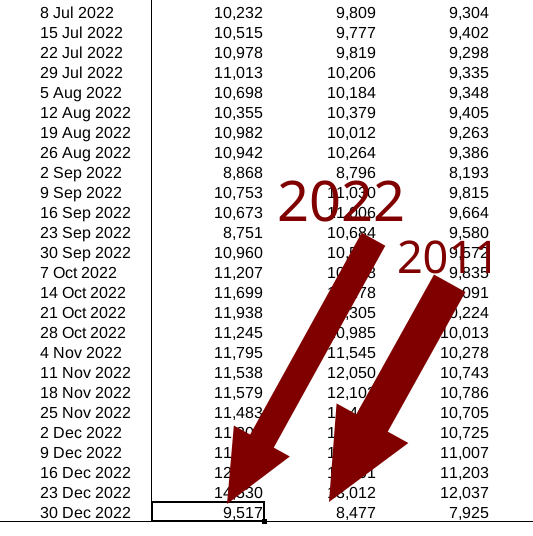
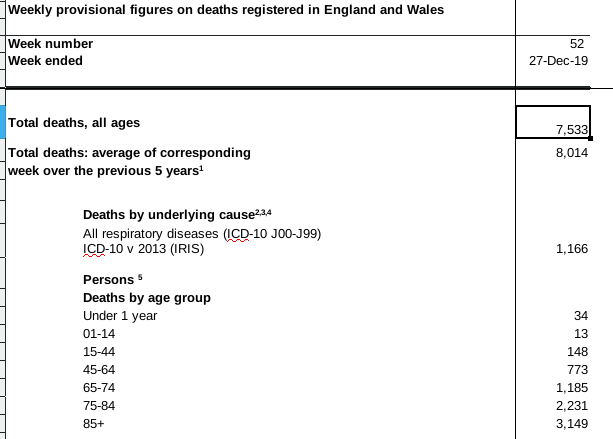
In your last update before Christmas you said clearly (in very large fonts) that there was an undercount, which was presented and contained in the datasheet. I took screenshots of that. 3 updates later, however, this number (undercount) has not been amended/corrected. Can you explain, clarify, rectify this? I wish to know what happened in the start of December when there was an undercount.
Kind regards,
If I receive a reply, I will share the gist of it or the whole thing. Depends on sensibilities. If they do not reply, I will ask again. These people are paid by us to inform us.
 AM by no means a
AM by no means a