England and Wales Deaths Rose From 9,867 to 11,241 in Six Years (Very Considerable Weekly Increase)
 Filed under:
Filed under:  T may seem repetitive, but this is still important. It’s also more relevant than ever, even if the media chooses to brush it under the rug.
T may seem repetitive, but this is still important. It’s also more relevant than ever, even if the media chooses to brush it under the rug.
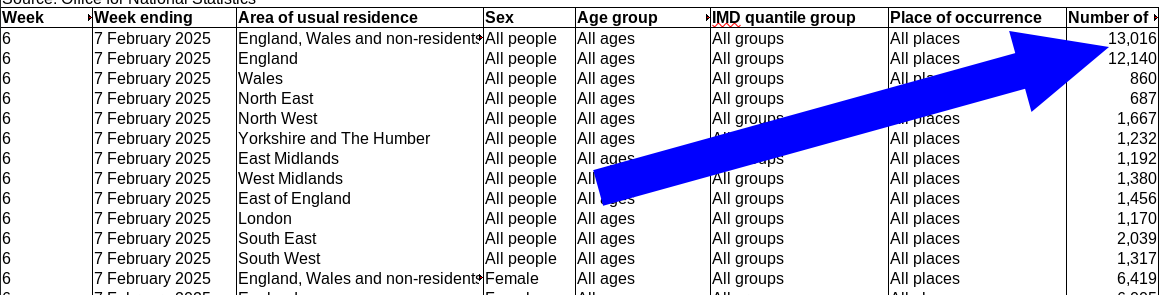
New ONS data came out this morning (in Microsoft’s proprietary format, as usual). 9,867 England and Wales deaths in Week 13 of 2019 compared to 11,241 in the same week this year.
It’s like this almost every week, including the prior week (12). I check this every Wednesday (for years already).
Is it OK to ask my government what has caused this very sharp increase?
Does it make one a “crank” for asking?
 HIS morning’s
HIS morning’s